




Findings
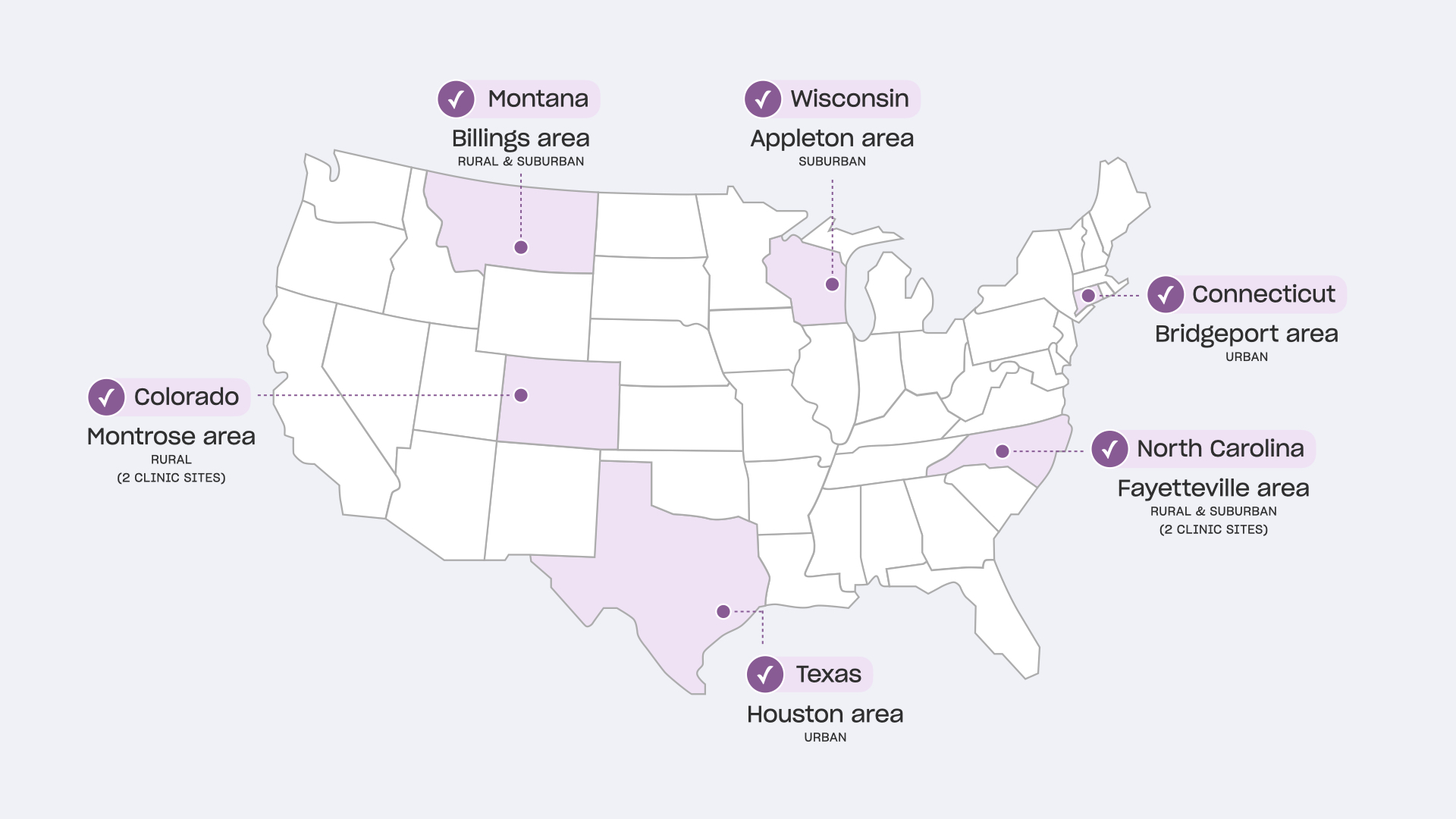
We analyzed 800+ data points from observations and interviews, 36 survey responses from participating parents/caregivers, and a variety of collected vaccine communication materials. Across the participating clinics, we observed patterns in how vaccine conversations were conducted, what materials were used, and which characteristics facilitated or created barriers to the vaccine conversations.
Clinical Vaccine Communication Flow

HCP Roles: Physicians/APPs tended to be the primary initiators of vaccine conversation. A distributed team involving receptionists, nurses, and medical assistants helped build trust with P/Cs before and after their interactions with their physician/APP. All play a critical role in sharing important vaccine safety information with families.
Conversation Duration and Timing: P/Cs without vaccine concerns had short vaccine conversations, ranging from 30 seconds to 3 minutes. For P/Cs with concerns, physicians/APPs spent more time addressing their questions, which extended the conversation time to 10-20 minutes. Vaccine conversations typically occurred during the middle or end of an appointment.
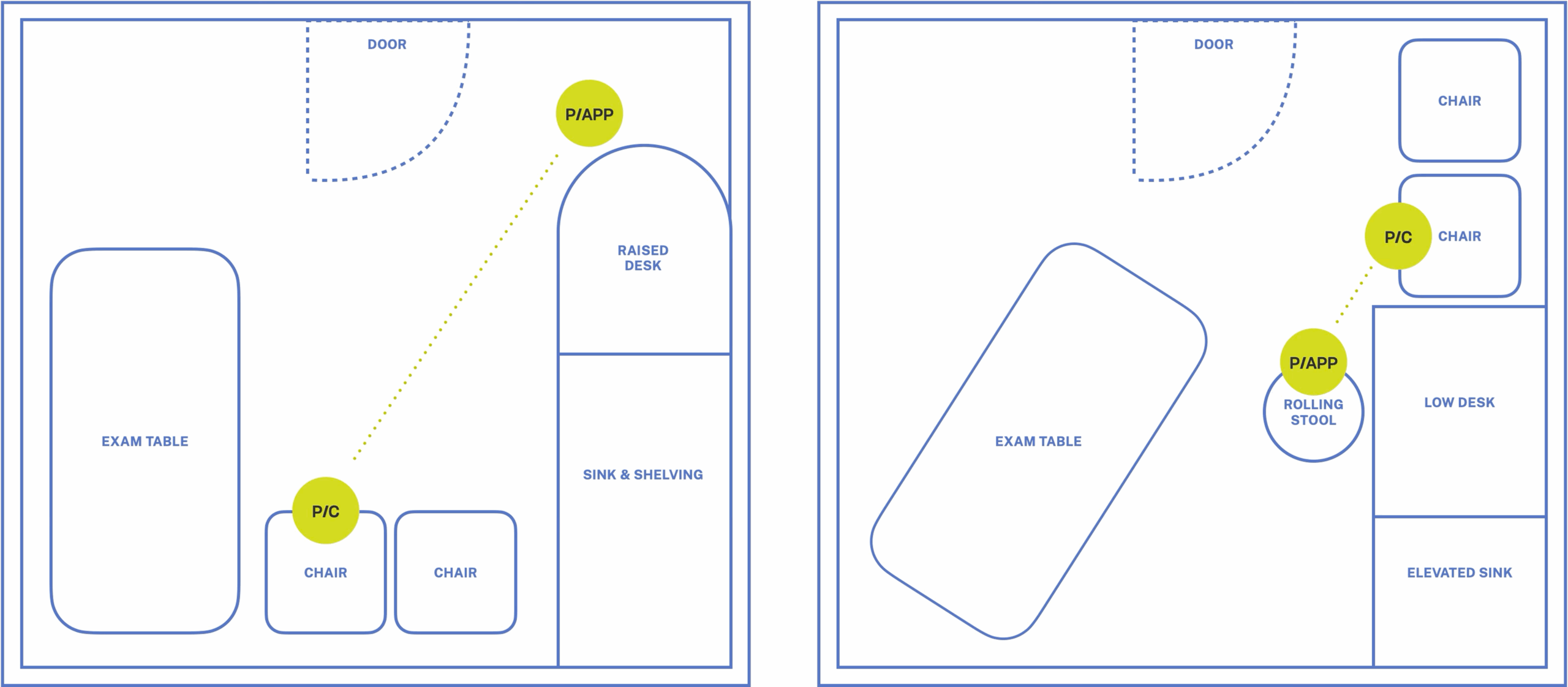
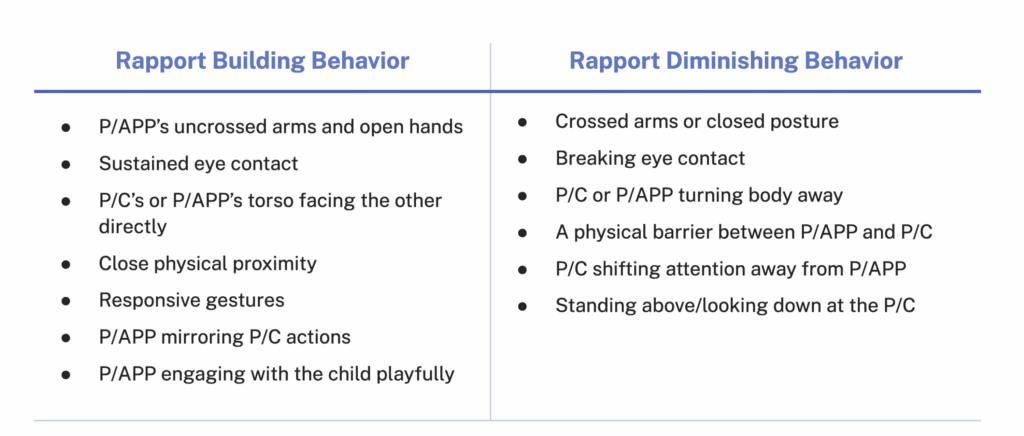
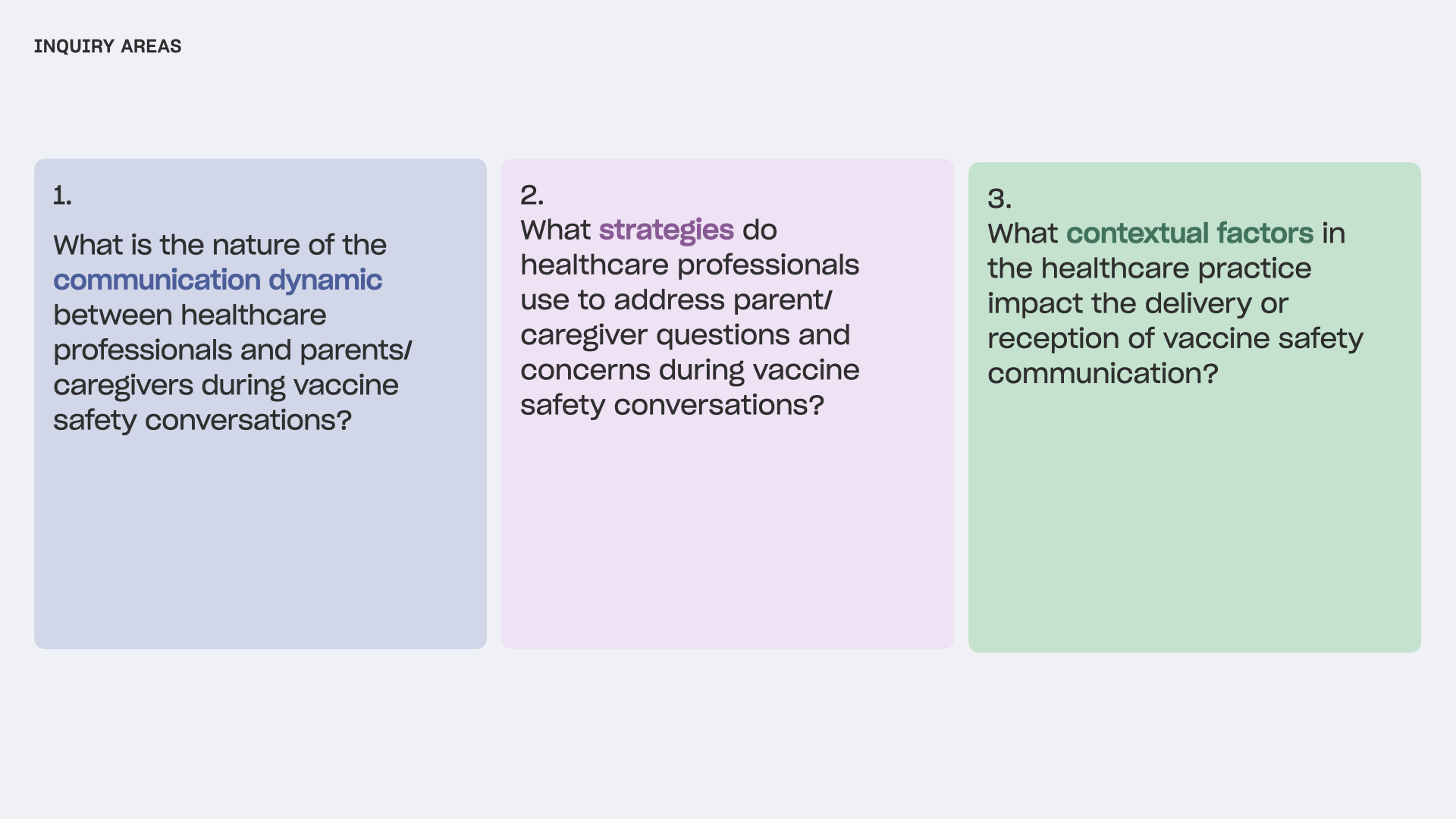
Communication Dynamic